

Breastfeeding can be challenging, especially in the early days. But remember that you are not alone. Lactation consultants can help you find ways to make breastfeeding work for you and your baby. Some women face many different problems while breastfeeding, while others do not. Also, many women may have certain problems with one baby that they don't have with their second or third baby.
Challenge: Sore nipples
Many moms say that their nipples feel tender when they first start breastfeeding. Breastfeeding should feel comfortable once you and your baby have found a good latch and some positions that work.
What you can do
- Your baby should not be suckling from just the nipple. The baby should be nursing from most of the areola (the darker colored area around the nipple) and the nipple.
- A good latch is key, so visit the Getting a good latch section for detailed instructions. If your baby sucks only on the nipple, gently break your baby's suction to your breast by placing a clean finger in the corner of your baby's mouth. Then try again to get your baby to latch on. (Your nipple should not look flat or compressed when it comes out of your baby's mouth. It should look round and long or the same shape as it was before the feeding.)
- If you find yourself putting off feedings because breastfeeding is painful, get help from a lactation consultant. Delaying feedings can cause more pain and harm your milk supply.
- Try changing positions each time you breastfeed. The Breastfeeding holds section describes the various positions you can try.
- Help cracked nipples stay moist so you can continue breastfeeding. Try one or all of these tips:
- After breastfeeding, express a few drops of milk and gently rub the milk on your nipples with clean hands. Human milk has natural healing properties and contains oils that soothe.
- Use purified lanolin cream or ointment that is especially made for breastfeeding.
- Let your nipples air dry after feeding, or wear a soft cotton shirt.
- Get help from your doctor or lactation consultant before using creams, hydrogel pads (a moist covering for the nipple to help ease soreness), or a nipple shield (a plastic device that covers the nipple during breastfeeding). In some cases, you should not use these products. Your doctor or lactation consultant will help you make the choice that is best for you.
- Don't wear bras or clothes that are too tight and put pressure on your nipples.
- Change nursing pads (washable or disposable pads you can place in your bra to absorb leaks) often to avoid trapping in moisture that can cause cracked nipples.
- Avoid harsh soaps or ointments that contain astringents (like a toner) on your nipples. Washing with clean water is all that is needed to keep your nipples and breasts clean.
If you have very sore nipples, you can ask your doctor about using non-aspirin pain relievers.
Challenge: Low milk supply
Most mothers make plenty of milk for their babies. But many mothers worry about having enough milk. This video suggests that checking your baby's weight and growth is the best way to make sure he or she gets enough milk. Let your baby's doctor know if you are concerned.
For more ways to tell if your baby is getting enough milk, visit the How do I know if my baby is getting enough breastmilk? section.
There may be times when you think your supply is low, but it is actually just fine:
- When your baby is around 6 weeks to 2 months old, your breasts may no longer feel full. This is normal. At the same time, your baby may nurse for only five minutes at a time. This can mean that you and your baby are just getting used to breastfeeding — and getting good at it!
- Growth spurts can make your baby nurse longer and more often. These growth spurts often happen around 2 to 3 weeks, 6 weeks, and 3 months of age. Growth spurts can also happen at any time. Don't be worried that your supply is too low to satisfy your baby. Follow your baby's lead. Nursing more and more often will help increase your milk supply. Once your supply increases, you will probably be back to your usual routine.
What you can do
- Make sure your baby is latched on and positioned well.
- Breastfeed often and let your baby decide when to end the feeding.
- Offer both breasts at each feeding. Have your baby stay at the first breast as long as he or she is still sucking and swallowing. Offer the second breast when the baby slows down or stops.
- Avoid giving your baby formula or cereal in addition to your breastmilk, especially in the first 6 months of life. Your baby may lose interest in your breastmilk, and your milk supply will decrease. If you need to supplement your baby's feedings with more milk, try using a spoon, cup, or a dropper filled with pumped breastmilk.
Check with your doctor for health issues, such as hormonal issues or primary breast insufficiency, if the above steps don't help.
Challenge: Oversupply of milk
An overfull breast can make breastfeeding stressful and uncomfortable for you and your baby.
What you can do
- Breastfeed on one side for each feeding. Continue to offer that same breast for at least two hours until the next full feeding, gradually increasing the length of time per feeding.
- If the other breast feels unbearably full before you are ready to breastfeed on it, hand express for a few moments to relieve some of the pressure. You can also use a cold compress or washcloth to reduce discomfort and swelling.
- Feed your baby before he or she becomes overly hungry to prevent aggressive sucking. (Learn about hunger signs in the Tips for breastfeeding success section.)
- Burp your baby often if he or she is gassy so there is more room in baby's tummy for milk.
Challenge: Strong let-down reflex
Some women have a strong milk ejection reflex or let-down. This can happen along with an oversupply of milk.
What you can do
- Hold your nipple between your first and middle fingers or with the side of your hand. Lightly press on milk ducts to reduce the force of the milk ejection.
- If your baby chokes or sputters when breastfeeding, unlatch him or her and let the extra milk spray into a towel or cloth.
- Allow your baby to latch and unlatch from the breast whenever he or she wants to.
- Try positions that reduce the force of gravity, which can make milk spray worse. These positions include the side-lying position and the football hold. (See the Breastfeeding holds section for illustrations of these positions.)
Challenge: Engorgement
It is normal for your breasts to become larger, heavier, and a little tender when they begin making milk. Sometimes, this fullness may turn into engorgement, when your breasts feel very hard and painful. Engorgement is the result of the milk building up. It usually happens during the third to fifth day after giving birth. But it can happen at any time, especially if you have an oversupply of milk or are not feeding your baby or expressing your milk often.
Engorgement can also cause:
- Breast swelling
- Breast tenderness
- Warmth
- Redness
- Throbbing
- Flattening of the nipple
- Low-grade fever
Engorgement can lead to plugged ducts or a breast infection, so it is important to try to prevent it before this happens.
What you can do
- Breastfeed often after giving birth. As long as your baby is latched on and sucking well, allow your baby to feed for as long as he or she likes.
- Work with a lactation consultant to improve your baby's latch so that your baby can remove more milk from your breast.
- Breastfeed often on the engorged side to remove the milk, keep the milk moving freely, and prevent your breast from becoming too full.
- Do not use pacifiers or bottles to supplement feedings in the beginning. Try to wait to introduce pacifiers until your baby is 3 or 4 weeks old.
- Hand express or pump a little milk to soften the breast, areola, and nipple before breastfeeding.
- Massage the breast.
- Use cold compresses on your breast in between feedings to help ease the pain.
- If you are returning to work, try to pump your milk on the same schedule that your baby breastfed at home. Pump at least every four hours, or more often.
- Get enough rest, proper nutrition, and fluids.
- Wear a well-fitting, supportive bra that is not too tight.
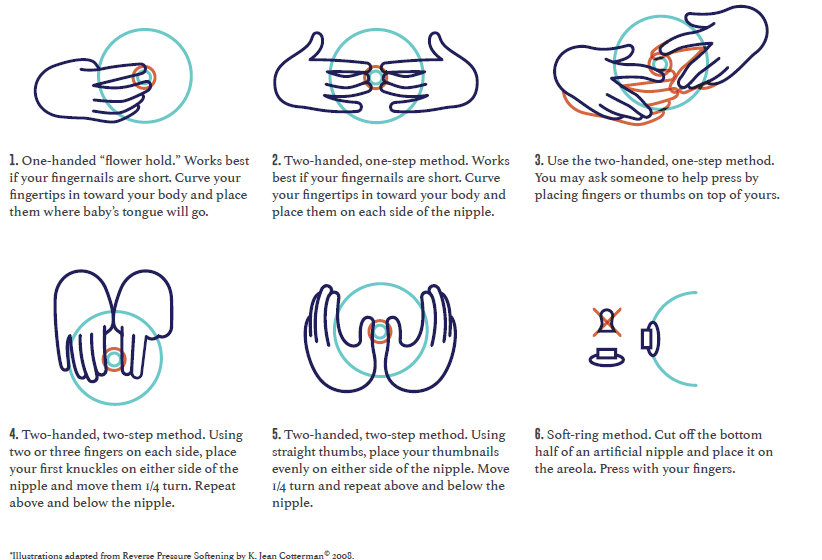
Try reverse pressure softening to make the areola soft around the base of the nipple and help your baby latch. Try one of the holds in the illustrations below. Press inward toward the chest wall and count slowly to 50. Use steady and firm pressure, but gentle enough to avoid pain. You may need to repeat each time you breastfeed for a few days.
- One-handed "flower hold." Works best if your fingernails are short. Curve your fingertips in toward your body and place them where baby's tongue will go.
- Two-handed, one-step method. Works best if your fingernails are short. Curve your fingertips in toward your body and place them on each side of the nipple.
- Two-handed, one-step method. You may ask someone to help press by placing fingers or thumbs on top of yours.
- Two-handed, two-step method. Using two or three fingers on each side, place your first knuckles on either side of the nipple and move them 1/4 turn. Repeat above and below the nipple.
- Two-handed, two-step method. Using straight thumbs, place your thumbnails evenly on either side of the nipple. Move 1/4 turn and repeat above and below the nipple.
- Soft-ring method. Cut off the bottom half of an artificial nipple and place it on the areola. Press with your fingers.
Challenge: Plugged ducts
Plugged ducts are common in breastfeeding mothers. A plugged milk duct feels like a tender and sore lump in the breast. If you have a fever or other symptoms then you probably have a breast infection rather than plugged ducts.
A plugged duct happens when a milk duct does not drain properly. Pressure then builds up behind the plug, and surrounding tissue gets inflamed. A plugged duct usually happens in only one breast at a time.
What you can do
- Breastfeed on the side with a plugged duct as often as every two hours. This will help loosen the plug and keep your milk moving freely.
- Aim your baby's chin at the plug. This will focus his or her suck on the duct that is affected.
- Massage the area, starting behind the sore spot. Move your fingers in a circular motion and massage toward the nipple. Use a warm compress on the sore area.
- Rely on others to help you get extra sleep, or relax with your feet up to help speed healing. Often a plugged duct is a sign that you are doing too much.
- Wear a well-fitting, supportive bra that is not too tight, since a tight bra can constrict milk ducts. Consider trying a bra without an underwire.
- If you have plugged ducts that keep coming back, get help from a lactation consultant.
Challenge: Breast infection (mastitis)
Mastitis (mast-EYE-tiss) is soreness or a lump in the breast. It can cause symptoms such as:
- Fever and/or flu-like symptoms, such as feeling run down or very achy
- Nausea
- Vomiting
- Yellowish discharge from the nipple that looks like colostrum
- Breasts that feel warm or hot to the touch and appear pink or red
A breast infection can happen when other family members have a cold or the flu. It usually happens in only one breast. It is not always easy to tell the difference between a breast infection and a plugged duct, because both have similar symptoms and can get better within 24 to 48 hours. Some breast infections that do not get better on their own need to be treated with prescription medicine from a doctor. (Learn more about medicines and breastfeeding in the Breastfeeding fact sheet.)
What you can do
- Breastfeed on the infected side every two hours or more often. This will keep the milk moving freely and your breast from becoming too full.
- Massage the area, starting behind the sore spot. Move your fingers in a circular motion and massage toward the nipple.
- Apply heat to the sore area with a warm, wet cloth.
- Rely on others to help you get extra sleep or relax with your feet up to help speed healing. Often a breast infection is a sign that you are doing too much and becoming overly tired.
- Wear a well-fitting, supportive bra that is not too tight, since a tight bra can constrict milk ducts.
Ask your doctor for help if you do not feel better within 24 hours of trying these tips, if you have a fever, or if your symptoms get worse. You might need medicine. See your doctor right away if:
- You have a breast infection in which both breasts look affected
- There is pus or blood in your breastmilk
- You have red streaks near the affected area of the breast
- Your symptoms came on severely and suddenly
Challenge: Fungal infections
A fungal infection, also called a yeast infection or thrush, can form on your nipples or in your breast. This type of infection thrives on milk and is an overgrowth of the Candida organism. Candida lives in our bodies and is kept healthy and at the correct levels by the natural bacteria in our bodies. When the natural balance of bacteria is upset, Candida can overgrow, causing an infection.
A key sign of a fungal infection is sore nipples that last more than a few days, even after your baby has a good latch. Or you may suddenly get sore nipples after several weeks of pain-free breastfeeding. Other signs are pink, flaky, shiny, itchy, or cracked nipples or deep pink and blistered nipples. You could also have achy breasts or shooting pains deep in the breast during or after feedings.
Causes of fungal infection include:
- Thrush in your baby's mouth, which can pass to you
- Nipples that are sore or cracked
- Receiving or taking antibiotics or steroids (often given to mothers during labor)
- A chronic illness like HIV, diabetes, or anemia
What you can do
Fungal infections are treated with a medicine you rub on your breasts several times a day for about a week. It may take several weeks to clear up, so it is important to follow these tips to avoid spreading the infection:
- Change disposable nursing pads often.
- Wash any towels or clothing that comes in contact with the yeast in very hot water (above 122°F).
- Wear a clean bra every day.
- Wash your hands often.
- Wash your baby's hands often, especially if he or she sucks on his or her fingers.
- Boil every day all pacifiers, bottle nipples, or toys your baby puts in his or her mouth. (To boil them, place them in a pot of water and heat the water to a rolling boil. Boil the items for about 10 minutes.)
- After one week of treatment, throw away all pacifiers and nipples and buy new ones.
- Every day, boil all breast pump parts that touch your milk.
- Make sure other family members do not have thrush or other fungal infections. If they have symptoms, do not let them care for you or your baby until they get treated.
Challenge: Inverted, flat, or very large nipples
Some women have nipples that turn inward instead of pointing outward or are flat and do not protrude. Nipples can also sometimes flatten for a short time because of engorgement or swelling from breastfeeding. Inverted or flat nipples can sometimes make it harder to breastfeed. For breastfeeding to work your baby must latch on to both the nipple and the breast, so even inverted nipples can work just fine. Often, flat and inverted nipples will protrude more over time as the baby sucks more.
Very large nipples can make it hard for the baby to get enough of the areola into his or her mouth to compress the milk ducts and get enough milk.
What you can do
- Talk to your doctor or a lactation consultant if you are concerned about your nipples.
- You can use your fingers to try to pull your nipples out. You can also talk to your doctor or nurse about using a device that gently suctions or pulls out inverted or temporarily flattened nipples.
- The latch for babies of mothers with very large nipples will improve with time as the baby grows. It might take several weeks to get the baby to latch well. But if you have a good milk supply, your baby will get enough milk even with a latch that isn't perfect.
Challenge: Nursing strike
A nursing "strike" is when your baby has been breastfeeding well for months and then suddenly begins to refuse the breast. A nursing strike can mean that your baby is trying to let you know that something is wrong. This usually does not mean that the baby is ready to wean (stop breastfeeding totally).
Not all babies will react the same way to the different things that can cause a nursing strike. Some babies will continue to breastfeed without a problem. Other babies may just become fussy at the breast. And other babies will refuse the breast entirely.
Some of the major causes of a nursing strike include:
- Having mouth pain from teething, a fungal infection like thrush, or a cold sore
- Having an ear infection, which causes pain while sucking or pressure while lying on one side
- Feeling pain from a certain breastfeeding position, perhaps from an injury on the baby's body or from soreness from an immunization
- Being upset about a long separation from the mother or a major change in routine
- Being distracted while breastfeeding, such as becoming interested in other things going on around the baby
- Having a cold or stuffy nose that makes breathing while breastfeeding difficult
- Getting less milk from the mother after supplementing breastmilk with bottles or overuse of a pacifier
- Responding to the mother's strong reaction if the baby has bitten her while breastfeeding
- Being upset by hearing arguing or people talking in a harsh voice while breastfeeding
- Reacting to stress, overstimulation, or having been repeatedly put off when wanting to breastfeed
If your baby is on a nursing strike, it is normal to feel frustrated and upset, especially if your baby is unhappy. Be patient with your baby and keep trying to offer your breasts. You may also want to pump your breastmilk to offer during the strike and to make sure you do not get engorged.
What you can do
- Try to hand express or pump your milk as often as the baby used to breastfeed, to prevent engorgement and plugged ducts.
- Try another feeding method temporarily to give your baby your breastmilk, such as using a cup, dropper, or spoon.
- Keep track of your baby's wet and dirty diapers to make sure he or she is getting enough milk.
- Keep offering your breast to your baby. If your baby is frustrated, stop and try again later. You can also try offering your breast when your baby is very sleepy or is sleeping.
- Try breastfeeding positions where your bare skin is pressed next to your baby's bare skin.
- Focus on your baby, and comfort him or her with extra touching and cuddling.
- Try breastfeeding while rocking your baby in a quiet room without distractions.
Did we answer your question about breastfeeding challenges?
For more information about breastfeeding challenges, call the OWH Helpline at 1-800-994-9662 or check out the following resources from other organizations:
- Breastfeeding — Information from the Centers for Disease Control and Prevention.
- Breastfeeding — Information from the U.S. Library of Medicine.
- Breastfeeding Your Baby — Resource from the American College of Obstetricians and Gynecologists.
- Colic and Crying — Fact sheet from the National Library of Medicine.
- Breastfeeding with Sore Nipples — Information from La Leche League International.
- Is Thrush Causing My Sore Nipples? — Information from La Leche League International.
- Mastitis — Information from La Leche League International.
- Overcoming Breastfeeding Problems — Information from the U.S. Library of Medicine.